It seems to becoming clear that in order to transition out of lock down a strategy of testing, tracing, isolating and quarantining (TTIQ), at scale, needs to be adopted. What is interesting is how “the science” around all this in the UK seems to evolve, almost in lock step, with the availability of the resources to implement the science. This helpfully means the Government can pretty much always do the right thing at the right time.
But how much testing needs to be done? To address this I guess one question is, what is testing for? From a lay persons point of view it seems to me there are broadly three purposes to testing.
First, a clinical one. This is about testing to identify which people, exhibiting serious symptoms are actually infected with Covid-19. The outcome of this being critical in determining the way the patient is managed.
Another clinical reason for testing is to check those managing the disease, working closely with patients and caring for the most vulnerable are not infected and thus in danger of spreading the disease. Ideally, I guess you would want to test front line staff perhaps once a week to ensure they are not working whilst infected but asymptomatic.
With these types of testing you would expect the ratio of positive to negative results as likely to be high. Essentially you are using self selected samples of most at risk people and therefore most likely to prove to have the disease. As of 9.00am on 30 April roughly 690k people had been tested and of those 170k tested positive which is almost 25% of those tested.
The second purpose for testing we might call epidemiological. It is about trying to understand the progress of the disease, its prevalence and spread, where the hot spots are etc. How effective this testing is will probably be critical to the design and success of any transition out of lock down.
This is what I take Pillar 4 of the testing regime to be partly about. Currently the numbers devoted to this are very low, just short of 10k out of the 690k tested to date. It may be that fancy sampling techniques means this is sufficient. However none of these random tests have so far proved positive so to a lay person this suggests a larger sample may be needed.
Given the 25% ratio between sampling and disease in the self selected groups mentioned above and the zero infection rate in the Pillar 4 sample you suspect there must be a Goldilocks sample size and structure that gives more useful information. One suspects the size of Pillar 4 sample is currently being determined by availability of tests rather than statistical design.
The third role for testing is “R” management. This is about running a “wack a mole” programme of early identification of potential carriers and trying to break the chain of infection, of which they are a link, as soon as possible.
We know when we come out of lock down the disease will still be with us, lurking in the community. Success will be about managing not eliminating infection. Keeping the “R” as low as possible, so those who contract the disease and require critical care do not overwhelm the NHS. Or indeed take up all available resource thus increasing the collateral, non Covid-19, mortality rate.
In lock down “R” was controlled by the radical separation of people. Confining them within their homes. The less opportunity people have to interact at all the less opportunity for the disease to spread. This does appear to have been effective but it is incredibly disruptive economically, socially and also, as time goes by, on people’s mental and physical health.
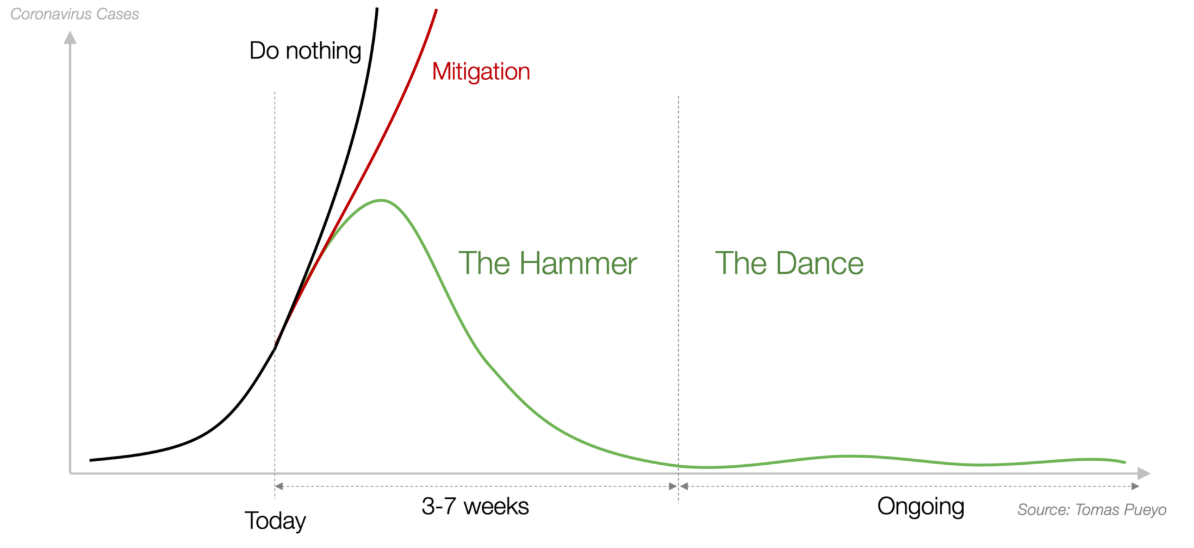
Having applied the hammer of lock down to get the “R” down to something below 1 we now need to look for more sophisticated ways of managing the spread to keep the “R” in check without lock down. Presumably when the R is above a certain level the only way to control it is through lock down. But when you get it below a certain level (something below 1) the progression of the disease is at least susceptible to less disruptive forms of management.
Social distancing protocols will be important in this but it is impossible they will be as effective as lock down so the virus will inevitably begin to spread again. This is where TTIQ at scale comes in, breaking the chain of infection as soon as the mole emerges into the light.
Ideally of course you would like to track it and intervene before it fully emerges into the light. To do this you would have to test everyone at least once a week to keep absolutely on top of the disease. That is 66m tests per week, 3.4bn tests a year. Mmm, probably not.
In the absence of this fanciful ideal what you need is a very agile and fast regime of TTIQ which responds immediately to individuals with even minimum symptoms, ideally supplemented with some large scale randomised tests to try and get ahead of the disease.
This means having significant numbers tests available and Test and Trace teams. Their job would be to go out as soon as someone identified as symptomatic, even if mild flu like symptoms, and test them. If the test was positive isolating those individuals and then tracing all of their contacts over, say, the past two weeks and ensuring those most at risk are tested and quarantined. For this, speed is obviously of the essence, as every day an infected person is not isolated they are spreading the disease.
TTIQ is foremost a logistical challenge. You need teams of well trained individuals with excellent interpersonal skill. Able to instantly respond to cases in the community, test the person, identify, trace, meet and test all their high risk contacts. Harvard Global Health Institute estimated an average of 10 tests of contacts per infected person.
Given all this how many Test and Trace teams would you need? That has to be a function of how many suspected cases are identified in the community per day. And how many cases a team can manage effectively per day. These are a couple of questions journalists might like to ask.
A related issue is the number of tests available to be used by the Test and Trace Teams. We should be up to 100,000 per day by now. Is that enough? In a recent blog, “Dancing out of lock down” I talked about research coming out of Harvard Global Health Institute suggesting a minimum number of tests as being of the order of 152 per 100k population. Which for the Uk seemed to work out at around 100k tests.
Whether this is right or not remains to be seen. An alternative estimate of the numbers needed comes from Tomas Pueyo who has now written a series of articles on the progress of Corvid-19 and how it is being managed. His latest is precisely about how to do testing. Initially I was cautious about Mr Pueyo’s credentials on this issue, however, over time I have found his common sense approach much more informative and convincing than the carefully honed statements of the UK press briefings.
Mr Pueyo argues sampling needs to be such as to ensure the proportion of positive outcomes is below 3%. This is what those countries which seem to have managed the disease well have done with early mass testing. Whilst I see the logic of his argument I guess this must be sensitive to the stage of the disease and thus general level of infection in the population. However, given all countries are probably at an early stage in this pandemic this is probably not a fatal criticism at the moment.
In the absence of statistically significant random testing identifying the level of “R” must involve working back from hospitalisation and death rates and some, no doubt, very clever epidemiological statistical manipulation.
The problem with this is you are looking backwards at the “R” rate which existed some days previously, and days matter. Fast and effective Test and Trace teams will not stop transmission of the disease but they may ensure, together with social isolation protocols, that its progress is reduced and the “R” kept within what the NHS can manage until we get a vaccine.
Throughout this blog so far I have talked about “the” “R” as if there is a single infection rate. This is not the case. Whilst the “R” in the general community seems to be managed by lock down it does not seem to be anywhere near as well managed in those communities that are locked in care and nursing homes and those locked up in prisons.
Urgent action needs to be taken to support these communities or what is a tragedy for those that live there, their carers and their families will become an ongoing source of infection in the wider community. We need to be able to see and address all the “R’s”
If increased resources are not supplied to these current hot spots, and a combination of social distancing and TTIQ do not slow the disease down enough, over time it will accelerate and we will have to resort, once again, to the blunderbuss which is lock down.
The World Health Organisations advice on managing this disease was “testing, testing, testing”. As the resources become available “the science” will show this is right and we will begin to do the “right thing at the right time” and see our “R’s”. The sooner the better.