
How do we get out of lockdown? Clearly the government are wrestling with the issue as we speak. They don’t want to share their thinking as they’re afraid the great British public are incapable of holding two ideas in their mind at the same time. Clearly, the government can draw on the advice of all manner of highly qualified professional advisors. And it is certain that whatever strategy eventually emerges will be guided by “the science”.
In what follows I attempt to think through some of the issues from a lay persons point of view. This is not to second guess what “the science” will show but to be able to ask sensible questions of the science when it emerges.
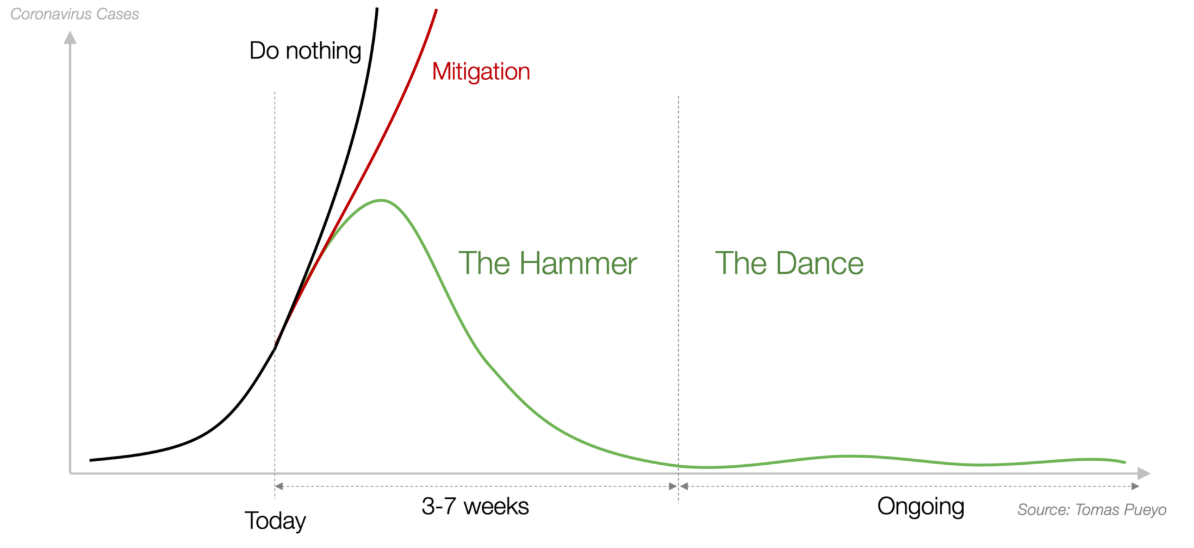
Some of the most consistently informative and convincing material I have read about Covid-19 has been that produced by Tomas Pueyo whose characterisation of the progression of the disease is particularly persuasive. He identifies basically two phases which he labels The Hammer and The Dance, illustrated below. In essence the Hammer is getting a grip of the disease and suppressing the spread. This is done through strict social distancing and lockdown. The Dance is where the lower rate of infection is maintained by retaining social distancing after lockdown but supplementing this with testing, tracing and isolation.
This process is inevitable in the absence of either a vaccine, a cure or herd immunity. All the evidence seems to be that the first two are unlikley to be available for some 12 to 18 months. This leaves herd immunity. However there are a series of problems with this.
First, it is not clear that individuals develop natural immunity. Second, even if we assume natural immunity is secured by infection and recovery then in a UK population of 66m people we need 39m to have contracted and survived the disease to get to the 60% personal immunity level needed for herd immunity.
How close are we to this number? In the absence of mass testing we can only guess at the number already infected. If we assume that the mortality rate is 1% of those infected as of when I started writing this (Saturday 18 April) the number of those that have died in the UK is reported as 15,464. This would suggest just over 1.5m people have the disease. [Warning this is uninformed common sense and may be something an epidemiologist would laugh at.] Logic says we therefore need another 27.5m to get infected and survive.
This brings us to the third problem, which is the cost in lives of securing herd immunity. In the absence of any treatment reducing the mortality rate, in order to get to herd immunity we might expect the ultimate death toll to be in excess of 390k people (1% of 39m). Without breaking the link between infection and mortality rate via a vaccine or cure these numbers look logical but unacceptable.
This would suggest a strategy is needed which buys us time. In other words reduces the number of deaths until a vaccine or cure is found. This can be done by: a) minimising the overall infection rate, the infamous “R” and; b) reducing the “R” even lower amongst the most vulnerable population. The initiatives to date by the government can be said to have been successful id a little late at dealing with a), however the picture on b) is rather mixed. The proposal that those who are particularly vulnerable should shelter at home makes sense to achieve b) however allowing the disease to get hold in care homes is the exact opposite.
So coming out of lock down what does the government need to do? It has set out a 5 point plan:
- Protect the NHS ability to provide sufficient critical care and specialist treatment across the UK;
- Need a sustained and consistent decline in the daily death rate;
- Reliable data that the infection rate or “R” is down to manageable levels across the board;
- Confident operational challenges, specifically testing and PPE are in hand;
- Confident no proposed change will risk a second peak in infection that overwhelms the NHS.
At the moment evidence seems to be building that the first three of Dominic Raab’s five tests for the movement out of lockdown will soon be met.
Test 1 is clearly a minimum requirement. Demand must be brought down to well within the capacity of the equipped and staffed ICU beds in the UK. Clearly the current level of demand is far too high. Demand needs to be reduced to a level which can accommodate spikes in demand, and the need to restart elective surgery and urgent cancer treatments. It also has to be at a level which does not put such an intolerable strain on front line staff.
However once you have got the disease down to a manageable level you need to turn to Mr Raab’s last two tests. These look sensible but rather problematic.
PPE remains a mess with the scale of the problem reducing the further away you get from the front line. It remains the case that for significant numbers of nurses, doctors and carers the lack of supply of PPE is an existential fear. Senior management, on the other hand, is confident there is sufficient PPE, although they are happy to change the guidelines on what PPE is appropriate mid-crisis, and not in a more stringent direction.
Which brings us to testing. Testing is the music needed for the Dance.
Matt Hancock has committed to achieving 100k tests per day by the end of April. At the moment the number of tests actually being done per day is around 20k. Matt Hancock says “Ahh yes, but there is capacity for 40k”. Unfortunately success is not measured by capacity but by results. I could have run a lot faster but I didn’t. Capacity is a necessary precondition of results but it is not sufficient. If we had infinite capacity to test everyone in Wick it would not be that much help. But put that aside.
Are 100k, actually completed, tests per day enough? It turns out they may be just about there if estimates of the level of testing needed to effectively monitor the disease post lockdown in the US, by the Harvard Global Health Institute, are correct. They suggest that a testing rate of a minimum of 152 tests per 100k population are needed to effectively monitor and manage the disease. Such a level should enable those showing any signs of disease, even mild flu like symptoms, to be tested in the community plus an average of 10 contacts.
Given a population of 66m divided by 100,000 gives you 660, multiplied by 152 = 100,320 tests per day required in the UK. Clearly there may be demographic or geographic or cultural drivers that move these numbers a bit but you would have thought they were in the right ballpark
So in order to go to the Dance without risking a second, unmanageable wave of infection, we need in place an infrastructure to enable a minimum of 100k tests per day to be carried out, all the contacts of those testing positive to be traced and all those infected isolated. A lot to put in place in less than three weeks.
Trying to draw some conclusions from all this.
First, what may delay coming out of lockdown is not the reduction in death rates etc it may be more about the materials and logistics for managing the virus after the end of lockdown.
Second, the end of lockdown is not the status quo ante. Far from. Our social, cultural and economic lives will continue to be severely constrained for some 12 to 24 months after the end of lockdown.
Third, this has specific economic consequences. Turning the economy off is a lot more straightforward than turning it back on. If the government does not continue to provide support to businesses in what might be a very long transition phase. more businesses could go bust coming out of lockdown than did going in.
Third, vulnerable groups are likely in for a particularly tough time. The reality may be they need to “shelter” until there is a vaccine. If this is the proposal from government it is not acceptable. They need to apply their minds to drive “the science” to come up with some way in which the vulnerable can get out of their homes, particularly those that live alone. Some creative thinking on this should be happening now and by pressure groups for the elderly and sick not just the scientists.
As Churchill might have put it coming out of lockdown is not the end, it’s not even the beginning of the end, it may however be the end of the beginning.
